
EMBER-3: A global Phase 3 trial in patients with ER+, HER2– MBC who are post AI (N=874)1,2
256 patients had ESR1m MBC (Arm A, n=138; Arm B, n=118)
Designed to test Inluriyo PFS vs fulvestrant or exemestane1,2

Schematic depicting the EMBER-3 trial design, which was designed to test Inluriyo PFS vs fulvestrant or exemestane in pre-menopausal women, postmenopausal women, and men with ER+, HER2− MBC. Patients were required to progress: On or ≤12 months of completing (neo)adjuvant AI therapy +/- CDK4/6i; or >12 months after (neo)adjuvant ET or de novo metastatic disease and progression on one line of AI +/- CDK4/6i. No other prior therapy was allowed for the treatment of MBC. Randomization was 1 to 1 to 1. The ESR1m MBC population (n=256), approved in a plasma specimen using an FDA-approved test, included Arm A: Inluriyo (n=138); and Arm B: investigator’s choice of fulvestrant (n=111) (one patient was randomized to Arm B and did not receive drug) or exemestane (n=6). Arm C was an investigational combination regimen.
Primary endpoints1,2
Secondary endpoints1,2
a Includes SERDs, chemotherapy, or PI3K pathway inhibitors.2
b Patients were treated until disease progression or unacceptable toxicity.1
cIn a plasma specimen using an FDA-approved test.1
dOne patient was randomized to Arm B and did not receive drug (fulvestrant).1
AI=aromatase inhibitor; BIRC=blinded independent review committee; CDK4/6i=cyclin-dependent kinase 4 and 6 dual inhibitor; ER+=estrogen receptor-positive; ESR1m=estrogen receptor-1-mutated; ET=endocrine therapy; FDA=Food and Drug Administration; HER2–=human epidermal growth factor receptor 2-negative; ITT=intent-to-treat; MBC=metastatic breast cancer; ORR=overall response rate; OS=overall survival; PFS=progression-free survival; PI3K=phosphatidylinositol 3-kinase; R=randomization; SERD=selective estrogen receptor degrader.
In a clinical trial studying patients with ER+, HER2–, ESR1m MBC (n=256)1,2
Inluriyo was studied across a wide range of patients1,2
Studied post AI in 1L and 2L MBC patients
Baseline demographics and characteristics in EMBER-31,2a
| Inluriyo (n=138) | Fulvestrant (n=111)b or exemestane (n=6) | ||
|---|---|---|---|
| Median age, yr (range) | 61 (28-85) | 60 (33-85) | |
| Postmenopausal status, n (%) | 122 (88.4) | 105 (89.0) | |
| ESR1m, n (%) | 138 (100.0) | 118 (100.0) | |
| PI3K pathway mutations,c n (%) | 72 (52.2) | 57 (48.3) | |
| Site of metastases, n (%) | |||
| Viscera | 84 (60.9) | 67 (56.8) | |
| Liver | 57 (41.3) | 47 (39.8) | |
| Bone only | 27 (19.6) | 30 (25.4) | |
| Most recent ET,d n (%) | |||
| As neoadjuvant or adjuvant therapy | 29 (21.0) | 23 (19.5) | |
| For MBC | 101 (73.2) | 91 (77.1) | |
Table depicting baseline demographics and characteristics in EMBER-3 for patients who received Inluriyo (n=138) or fulvestrant (n=111) or exemestane (n=6) (one patient was randomized to Arm B and did not receive drug (fulvestrant); percentages may not total 100 because of rounding):
- Median age, years (range): Inluriyo: 61 (28-85); fulvestrant or exemestane: 60 (33-85)
- Postmenopausal status, n (%): Inluriyo: 122 (88.4); fulvestrant or exemestane: 105 (89.0)
- ESR1m, n (%): Inluriyo: 138 (100.0); fulvestrant or exemestane: 118 (100.0)
- PI3K pathway mutations (included single nucleotide variants and insertions or deletions in the genes PIK3CA, AKT1, or PTEN as analyzed by Guardant360 ctDNA assay. This analysis excluded 40 patients from China and 18 patients with unknown ESR1-mutation status), n (%): Inluriyo: 72 (52.2); fulvestrant or exemestane: 57 (48.3)
- Site of metastases, n (%)
- Viscera: Inluriyo: 84 (60.9); fulvestrant or exemestane: 67 (56.8)
- Liver: Inluriyo: 57 (41.3); fulvestrant or exemestane: 47 (39.8)
- Bone only: Inluriyo: 27 (19.6); fulvestrant or exemestane: 30 (25.4)
- Most recent ET, n (%)
- As neoadjuvant or adjuvant therapy: Inluriyo: 29 (21.0); fulvestrant or exemestane: 23 (19.5)
- For MBC: Inluriyo: 101 (73.2); fulvestrant or exemestane: 91 (77.1)
a Percentages may not total 100 because of rounding.2
b One patient was randomized to Arm B and did not receive drug (fulvestrant).1
c PI3K pathway mutations included single nucleotide variants and insertions or deletions in the genes PIK3CA, AKT1, or PTEN as analyzed by Guardant360 ctDNA assay. This analysis excluded 40 patients from China and 18 patients with unknown ESR1-mutation status.2
d Prior endocrine therapy for 1L patients was in the adjuvant setting; prior endocrine therapy for 2L patients was in the advanced setting.2
1L=first line; 2L=second line; AI=aromatase inhibitor; AKT1=protein kinase B alpha gene; ctDNA=circulating tumor DNA; ER+=estrogen receptor-positive; ESR1m=estrogen receptor-1-mutated; ET=endocrine therapy; HER2–=human epidermal growth factor receptor 2-negative; MBC=metastatic breast cancer; PI3K=phosphatidylinositol-3 kinase; PIK3CA=phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha gene; PTEN=phosphatase and tensin homolog gene.

In patients with ER+, HER2−, ESR1m MBC (n=256)1
Inluriyo provided superior PFS benefit vs fulvestrant or exemestane1
Investigator-assessed PFS in patients with ESR1m MBC1

Kaplan-Meier curve depicting the results of the EMBER-3 primary endpoint—investigator-assessed PFS—in patients who received Inluriyo (n=138) vs patients who received fulvestrant (n=111) or exemestane (n=6). Median PFS was 5.5 months with Inluriyo vs 3.8 months with fulvestrant or exemestane (HR=0.62 [95% CI: 0.46-0.82]); P=0.0008. The number of patients at risk with Inluriyo vs fulvestrant or exemestane, respectively, was 138 vs 118 at Month 0; 95 vs 74 at Month 2; 74 vs 51 at Month 4; 56 vs 33 at Month 6; 45 vs 19 at Month 8; 35 vs 7 at Month 10; 22 vs 5 at Month 12; 18 vs 3 at Month 14; 15 vs 2 at Month 16; 8 vs 1 at Month 18; 4 vs 0 at Month 20; 4 vs 0 at Month 22; 3 vs 0 at Month 24; and 2 vs 0 at Month 26.
Inluriyo led to a 38% reduction in the risk of progression or death.1
Primary endpoint was met: 5.5 months mPFS with Inluriyo (n=138) vs 3.8 months mPFS with fulvestrant (n=111) or exemestane (n=6) (HR=0.62 [95% CI: 0.46-0.82]); P=0.0008.1*
*One patient was randomized to Arm B and did not receive drug (fulvestrant).1
Inluriyo maintained longer mPFS vs fulvestrant or exemestane with longer follow-up.1,3
At updated efficacy analysis (28.5 months follow-up): 5.5 months mPFS with Inluriyo (n=138) vs 3.8 months mPFS with fulvestrant (n=111) or exemestane (n=6) (HR 0.62 [95% CI: 0.47-0.82]).3
Updated PFS results based on the OS interim analysis (data cut-off: 18 August 2025) are descriptive only.
CI-confidence interval; HR=hazard ratio; mPFS=median progression-free survival; OS=overall survival; PFS=progression-free survival
Updated secondary endpoint: OS with Inluriyo vs fulvestrant or exemestane (50% maturity) 1,3
At the time of updated efficacy analysis, OS data were immature with 50% of deaths in the ESR1m population1,3a
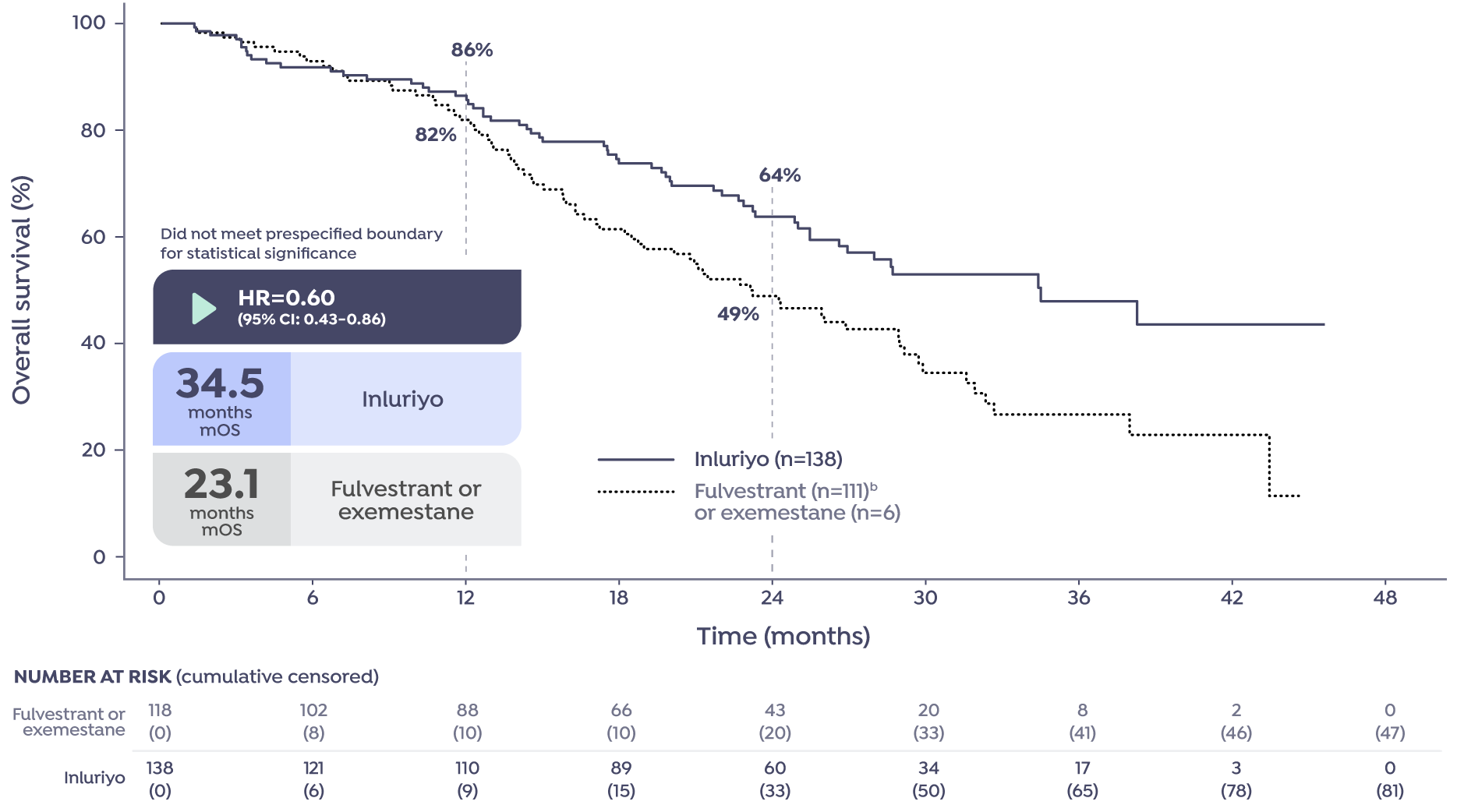
Kaplan-Meier curve depicting the updated results of the EMBER-3 secondary endpoint OS in patients who received Inluriyo (n=138) vs patients who received fulvestrant (n=111) or exemestane (n=6) (one patient was randomized to Arm B and did not receive drug (fulvestrant)). Median OS was not reached with Inluriyo (HR=0.60 [95% CI: 0.43-0.86]); this analysis did not achieve the prespecified threshold for significance. The number of patients at risk with Inluriyo vs fulvestrant or exemestane, respectively, was 138 vs 118 at Month 0; 121 vs 102 at Month 6; 110 vs 88 at Month 12; 89 vs 66 at Month 18; 60 vs 43 at Month 24; 34 vs 20 at Month 30; 17 vs 8 at Month 36; 3 vs 2 at Month 42; and 0 vs 0 at Month 48. The cumulative censored number of patients at risk with Inluriyo vs fulvestrant or exemestane, respectively, was 0 vs 0 at Month 0; 6 vs 8 at Month 6; 9 vs 10 at Month 12; 15 vs 10 at Month 18; 33 vs 20 at Month 24; 50 vs 33 at Month 30; 65 vs 41 at Month 36; 78 vs 46 at Month 42; and 81 vs 47 at Month 48.
A graphical testing procedure evaluated OS for statistical significance only if the corresponding PFS was statistically significant. This prespecified interim efficacy analysis (data cut-off: 18 August 2025) was triggered after ∼255 OS events had occurred among patients in the imlunestrant and comparator arms.3
At the time of primary outcome analysis, overall survival data were immature with 31% of deaths in the ESR1m population.1
aMedian follow-up: 29.5 months.3
bOne patient was randomized to Arm B and did not receive drug (fulvestrant).1
AI=aromatase inhibitor; CI=confidence interval; ER+=estrogen receptor-positive; ESR1m=estrogen receptor-1–mutated; ET=endocrine therapy; HER2–=human epidermal growth factor receptor 2-negative; HR=hazard ratio; mOS=median overall survival; OS=overall survival; PFS=progression-free survival
In patients with ER+, HER2–, ESR1m MBC (n=256)1
Inluriyo time to chemotherapy in patients with ESR1m MBC3
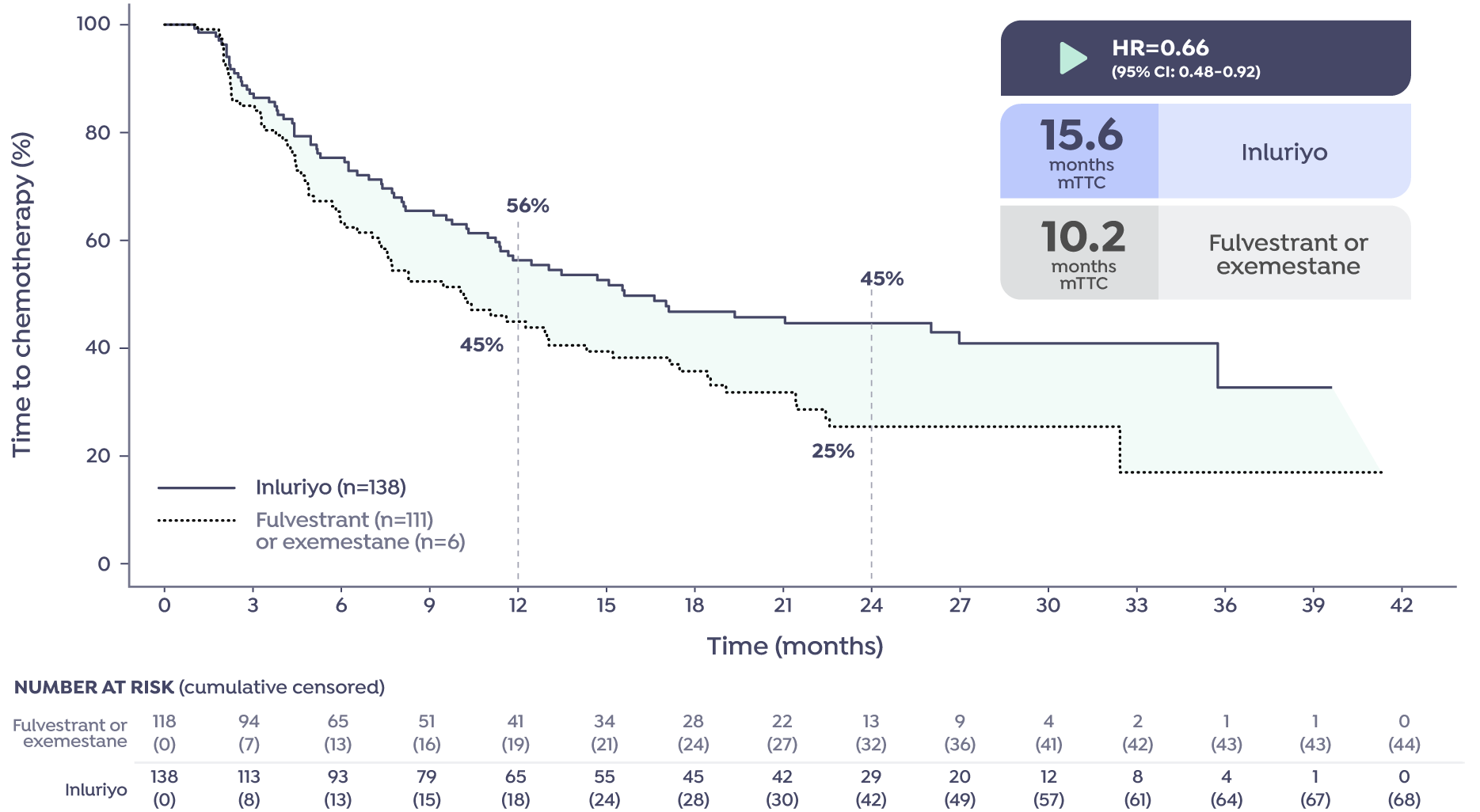
Kaplan-Meier curve depicting the results of the EMBER-3 exploratory endpoint time to chemotherapy (TTC) in patients who received Inluriyo (n=138) vs patients who received fulvestrant (n=111) or exemestane (n=6) (one patient was randomized to Arm B and did not receive drug (fulvestrant)). Median TTC was 15.6 months with Inluriyo vs 10.2 months with fulvestrant or exemestane (HR=0.66 [95% CI: 0.48-0.92]). The number of patients at risk with Inluriyo vs fulvestrant or exemestane, respectively, was 138 vs 118 at Month 0; 113 vs 94 at Month 3; 93 vs 65 at Month 6; 79 vs 51 at Month 9; 65 vs 41 at Month 12; 55 vs 34 at Month 15; 45 vs 28 at Month 18; 42 vs 22 at Month 21; 29 vs 13 at Month 24; 20 vs 9 at Month 27; 12 vs 4 at Month 30; 8 vs 2 at Month 33; 4 vs 1 at Month 36; 1 vs 1 at Month 39; and 0 vs 0 at Month 42. The cumulative censored number of patients at risk with Inluriyo vs fulvestrant or exemestane, respectively, was 0 vs 0 at Month 0; 8 vs 7 at Month 3; 13 vs 13 at Month 6; 15 vs 16 at Month 9; 18 vs 19 at Month 12; 24 vs 21 at Month 15; 28 vs 24 at Month 18; 30 vs 27 at Month 21; 42 vs 32 at Month 24; 49 vs 36 at Month 27; 57 vs 41 at Month 30; 61 vs 42 at Month 33; 64 vs 43 at Month 36; 67 vs 43 at Month 39; and 68 vs 44 at Month 42.
Exploratory endpoint: 15.6 months mTTC with Inluriyo (n=138) vs 10.2 months with fulvestrant (n=111) or exemestane (n=6) (HR=0.66 [95% CI: 0.48-0.92]).3*
Is TTC a consideration in your clinical decision making?
TTC was a prespecified exploratory endpoint and was not controlled for type I error. TTC was defined as the time from randomization to the start of the first chemotherapy (censoring patients who died before initiation of chemotherapy). Protocol did not dictate any requirements for subsequent therapy post study discontinuation. This prespecified interim efficacy analysis (data cut-off: 18 August 2025) was triggered after ∼255 OS events had occurred among patients in the imlunestrant and comparator arms.3
*One patient was randomized to Arm B and did not receive drug (fulvestrant).1
Cl=confidence interval; ER+=estrogen receptor-positive; ESR1m=estrogen receptor-1-mutated; HER2–=human epidermal growth factor receptor 2-negative; HR=hazard ratio; MBC=metastatic breast cancer; mTTC=median time to chemotherapy; OS=overall survival; TTC=time to chemotherapy
SELECT IMPORTANT SAFETY INFORMATION: WARNINGS AND PRECAUTIONS — EMBRYO-FETAL TOXICITY
Based on findings in animals and its mechanism of action, Inluriyo can cause fetal harm when administered to a pregnant woman. In an animal reproduction study, oral administration of imlunestrant to pregnant rats during the period of organogenesis led to embryo-fetal mortality and structural abnormalities at maternal exposures that were below the human exposure at the recommended dose based on area under the curve (AUC). Avoid the use of imlunestrant in pregnant women. Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential and males with female partners of reproductive potential to use effective contraception during treatment with Inluriyo and for 1 week after the last dose.
Quality of Life scores for patients with ESR1m MBC on Inluriyo and fulvestrant or exemestane4,5*†
This analysis was not prespecified. This was an exploratory analysis, with no control for type-1 error. This analysis is not a comparison between treatment arms.
Inluriyo and fulvestrant or exemestane in patients with ER+, HER2−, ESR1m MBC who were previously treated with ET4,5

Plot diagram of within-group least squares mean (SE) change from baseline in Global Health Status/Quality of Life, calculated using longitudinal mixed model for repeated measures with an unstructured covariance matrix. Improvement from baseline is represented by positive LS mean change values and worsening from baseline is represented by negative LS mean change values.
The analysis includes patients with baseline and post-baseline values for cycles in which at least 25% of patients in each arm have data.
*Global Health Status/Quality of Life as measured by EORTC QLQ-C30.
†The GHS/QoL domain of the EORTC QLQ-C30 contains 2 items. The raw scores of the 2 items are combined and transformed to a 0-100 score, with a higher score indicating better health status.
ER+=estrogen receptor-positive; ESR1m=estrogen receptor-1–mutated; GHS=Global Health Status; EORTC=European Organisation For Research And Treatment Of Cancer; ET=endocrine therapy; HER2–=human epidermal growth factor receptor 2-negative; LS=least squares; MBC=metastatic breast cancer; QLQ-C30=Quality of Life Questionnaire, Core 30; QoL=Quality of Life; SE=standard error.
References:
- Inluriyo. Prescribing Information. Lilly USA, LLC.
- Jhaveri KL, Neven P, Casalnuovo ML, et al. Imlunestrant with or without abemaciclib in advanced breast cancer. N Engl J Med. 2025;392(12):1189-1202. doi:101056/NEJMoa2410858
- Jhaveri KL, Neven P, Casalnuovo ML, et al. Imlunestrant with or without abemaciclib in advanced breast cancer: updated efficacy results from the phase III EMBER-3 trial. Ann Oncol. 2025;Epub(Incl suppl mat). doi:10.1016/j.annonc.2025.11.018
- Data on File. DOF-IN-US-0008. Lilly USA, LLC.
- Curigliano G, O'Shaughnessy J, Bidard FC, et al. Patient-reported outcomes (PROs) in patients with ER+, HER2– advanced breast cancer (ABC) treated with imlunestrant, investigator’s choice standard endocrine therapy, or imlunestrant + abemaciclib: results from the phase III EMBER-3 trial [abstract]. J Clin Oncol. 2025;43(Suppl 16):1001. doi:10.1200/JCO.2025.43.16_suppl.1001